
Robert Mayer remembers the attitude that cancer doctors had about pancreatic cancer when he first started practicing medicine in 1969:
“The disease represented a hopeless situation,” Mayer said. “I particularly recall a reasonable number of physicians in whom the diagnosis was made and they themselves were reluctant to undergo any form of treatment.”
Pancreatic cancer has been viewed as “an enormous scourge in the field of oncology,” said Mayer, who is now the faculty vice president for Academic Affairs at Dana-Farber Cancer Institute and faculty associate dean for Admissions at Harvard Medical School. Mayer appeared on this episode of The Cancer History Project Podcast.
When Mayer entered the clinic, the landscape of pancreatic cancer diagnosis and treatment was dismal.
“Making a diagnosis of pancreatic cancer often was restricted to the presence of metastatic disease because there was no scan, no blood test that showed that there was something awry in the pancreas. It was in the back of the abdomen,” Mayer said. “And that didn’t change for quite some time. So the aura developed that this was something that just you couldn’t deal with.”
In the forthcoming decades, he said, that attitude had remained largely unchanged.
That is until earlier this year when Revolution Medicines announced the results of the RASolute-302 trial results evaluating the pan-RAS(on) inhibitor daraxonrasib. The full results were presented at the 2026 American Society of Clinical Oncology annual meeting plenary session on May 31 (The Cancer Letter, June 5, 2026).
“The presentation that we heard about an effective RAS inhibitor we heard in ASCO several weeks ago dispels that notion,” Mayer said. “It tells us that pancreatic cancer, just as was once the case with melanoma, with renal cell cancer, may turn out to be treatable utilizing tools that we didn’t even know existed not so long ago.”
This episode is available on Spotify, Apple Podcasts, and YouTube.
For the first time in his 50-year career, Mayer felt a surge of hope for the future of pancreatic cancer.
The same is true for his colleagues. A tidal wave of hope electrified the room at the ASCO plenary, culminating in an eruption of applause that brought people to their feet in a resounding standing ovation as the Kaplan-Meier survival graph was projected on the big screens, showing that overall survival nearly doubled for patients with metastatic pancreatic cancer versus chemotherapy. (The Cancer Letter, June 5, 2026).
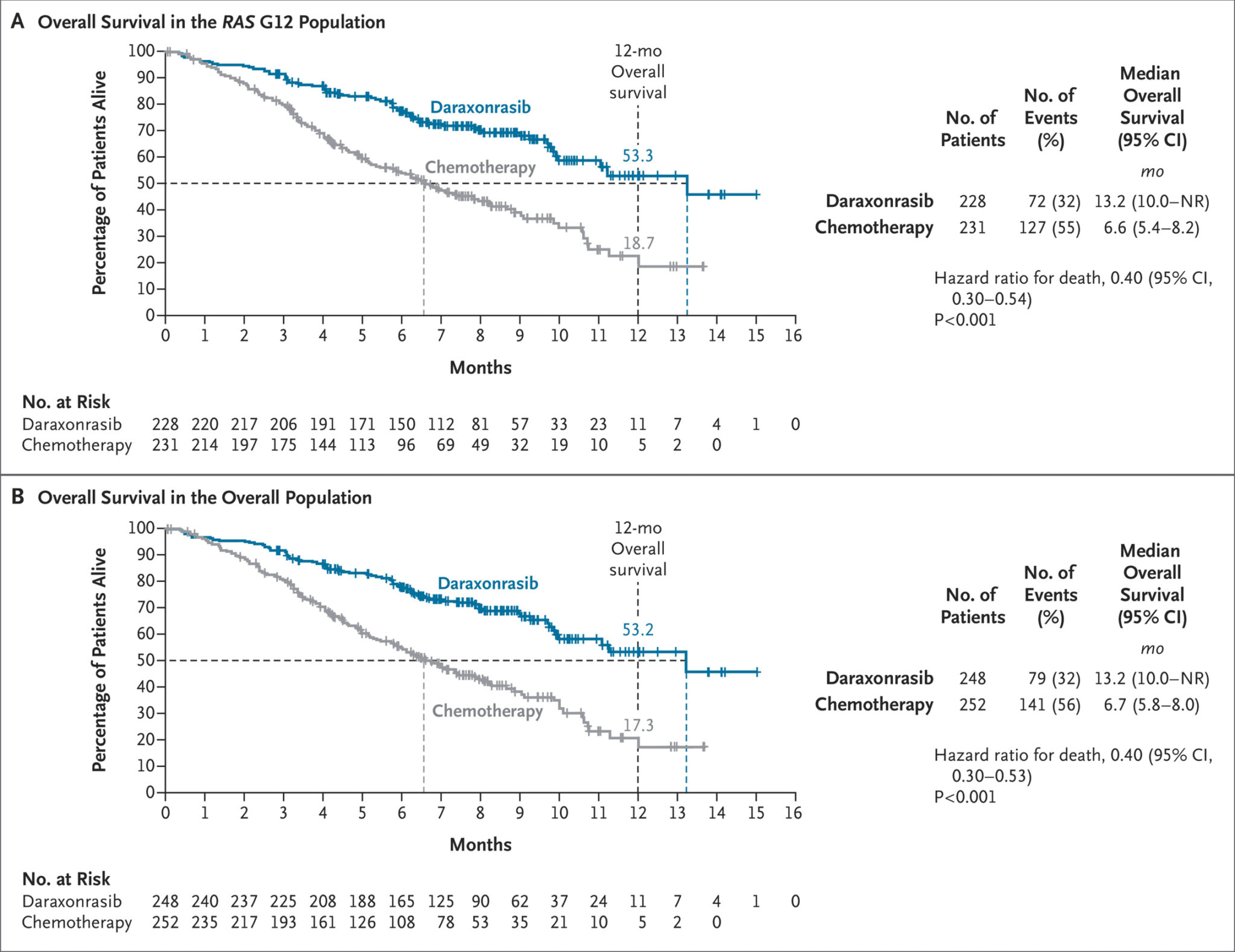
Mayer says the graph passed the “two finger rule.”
“I used to be on an editorial board, where the editor-in-chief said, ‘If you’re comparing two survival curves and you can’t put two fingers between them, statistics don’t matter. It has no clinical real bearing,’” Mayer said. “This is a whole fist, your whole hand [can fit] between the two curves.”
Calcified over many years—the “hopeless” attitude around pancreatic cancer is beginning to soften, Mayer said.
“As with other conditions that we treat, when patients [with pancreatic cancer] come, we’ll be able to give them options, plans, steps,” Mayer said. “It may not necessarily be that we can cure, but we can prolong survival, enhance quality of life, reduce time that they have to come to receive toxic systemic parenteral intravenous therapy. All things that really matter so that they can go and be at high school, college graduations, family celebrations, and do all the things that they otherwise would like to do. That has never been something that happened with pancreas cancer.”
Swings, misses, and foul balls
The development of daraxonrasib did not happen overnight. The discovery was built on the back of decades of research, federal funding, partnerships between government, academia, and industry, and tireless trial and error, Mayer said.
“I think it’s important for us all to appreciate that the observation about the efficacy of this new RAS inhibitor didn’t occur by accident,” Mayer said. “This is something that comes from years and years of swings, misses, foul balls, and finally a direct hit that really will—I very much believe—change the outcome for patients in the future with this disease.”
In the 1970s, Mayer was an investigator part of the NCI-supported Gastrointestinal Tumor Study Group, which was tasked with researching GI cancers, as well as pancreatic cancer. Compared to today’s standards, these researchers were arguably rummaging in the dark, developing and testing hypotheses without modern tools like CT scans.
Mayer recounts early discoveries, including that of the presence of desmoplastic scarring sheets that seem to protect tumors from radiation or surgery, that incrementally increased the field’s understanding of the cancer’s biology. But treatment improvements were stubbornly elusive.
“We still don’t have an answer for that, but that explained in some ways why radiation treatment was not as effective here as it was in colon cancer,” Mayer said.
Another step forward: the association between pancreatic cancer and diabetes, suggesting irritation and inflammation in the pancreas.
In 1982, three different labs, run by Mariano Barbacid, Robert Weinberg, and Michael Wigler, sequenced the HRAS oncogene. Quickly after, the lab of Geoffrey Cooper discovered a second transforming sequence called KRAS.
Scientists later learned that more than 90% of pancreatic ductal adenocarcinoma have the KRAS gene mutation (The Cancer Letter, Oct. 10, 2025).
“It was tantalizing to think that inhibiting that might do something beneficial for patients so afflicted, but a decade or more of a tense at developing inhibitors of the KRAS gene that would have any effect on pancreatic cancer turned out not to be fruitful and the RAS mutation of pancreatic cancer developed the reputation as being undruggable,” Mayer said.
That assumption would eventually prove incorrect. Before that revelation, scientists focused on other types of treatments with varying success.
In the 1990s, scientists developed gemcitabine, which later spurred drug combinations with nab-paclitaxel and abraxane. In the 2010s, investigators developed FOLFIRINOX, a chemotherapy regimen made of drugs that were being used to treat colon cancer at the time.
All these discoveries were steps on the path toward a RAS inhibitor that had substantial activity in pancreatic cancer.
“There’s nothing mystical about how science is conducted. It’s a long slog of wonderfully committed, amazingly talented people who collaborate,” Mayer said. “I know that many of the efforts that they undertake are not going to be successful, but [I see it as part of] the goal of improving the health of the people we serve. Now more than ever, the recognition of the support of fundamental basic research as the starting point for what will prove to be hopefully a major change in the outcome for patients with a dreaded disease has to continue and we as a society need to embrace that.”
Extending the survival graph
Daraxonrasib’s ability to double survival is a major milestone, but it isn’t a cure for pancreatic cancer.
Mayer says the work ahead consists of refining the treatment protocol of daraxonrasib, or other RAS inhibitors that could be around the corner.
“Now the issue of what happens if you give the RAS inhibitor before an operation?” Mayer questioned. “Could you shrink the tumor? Could you convert somebody who would otherwise be destined to recur or have an incomplete operation? Could you give the drug after the operation as well? What happens if you fail or the disease returns? Is this the only RAS inhibitor of its class?
“We certainly learned in the world of lung cancer and in the world of CML, chronic myelogenous leukemia, that the first drug that seemed to work didn’t necessarily represent the best that would ever come. On the other hand, it opened the door to new things and those new things have been amazing to watch.”
The only pathway forward is more trial and error, and more funding to support the investigation of these questions, Mayer says.
“I think the hors d’oeuvre table has a lot of options here, and I’m hoping that a lot of young, bright people who are entering this field will see this as a wonderful opportunity for us to move forward,” Mayer said.
Read more on The Cancer History Project. This interview is available on Spotify, Apple Podcasts, and YouTube.
Related Articles:
- Pancreatic cancer finally starts to budge as daraxonrasib doubles overall survival, June 5, 2026
- The story of daraxonrasib is the ultimate hero’s journey, June 5, 2026
- Long-awaited results from first phase III trial of a RAS inhibitor in pancreatic cancer shows that daraxonrasib doubles median OS, April 17, 2026
- KRAS pioneer and Stephenson Prize winner Frank McCormick aims to prevent all KRAS cancers with a pill, October 10, 2025
Episode Transcript:
Sara Willa Ernst: Robert Mayer first started practicing medicine in 1969. He is now the faculty vice president for Academic Affairs at Dana-Farber Cancer Institute and faculty associate dean for Admissions at Harvard Medical School.
And for the past 50 years, he says the attitude surrounding pancreatic cancer was hopelessness. And that has largely remained the case over the decades.
That’s until the curve began to budge this year. Revolution Medicines published the results of RASolute-302 phase III trial evaluating daraxonrasib, a RAS inhibitor. The results scientists presented at ASCO in May showed that overall survival doubled for patients with metastatic pancreatic cancer.
And the Kaplan-Meier survival graph inspired a resounding standing ovation that lasted 43 seconds during the presentation.
But this didn’t happen overnight. Dr. Mayer says there were many failed attempts to arrive here.
On this episode of The Cancer History Project Podcast, Dr. Mayer runs through the trial and errors, the smaller discoveries, and the incremental progress that got us to this breakthrough.
The Cancer History Project Podcast is sponsored by City of Hope, the American Society of Clinical Oncology, the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, and the University of Texas MD Anderson Cancer Center.
Katie Goldberg: The Cancer History Project is an online archive of the history of oncology collaboratively curated by the institutions and people who shaped it. We have over 60 partners spanning academic cancer centers, government agencies, advocacy groups, and even the occasional podcast. Visit us online at cancerhistoryproject.com to dig through our archives. I’m your host, Katie Goldberg.
Jacquelyn Cobb: Well, hello, Dr. Mayer. Thank you so much for taking the time to speak with me today. We have a long conversation hopefully in store where we’re going to be talking about daraxonrasib, which I’m still not perfect at pronouncing, but it has recently taken the oncology world by storm, being the first RAS inhibitor to show a really significant effect in pancreatic cancer and the first drug that really made a real dent in metastatic pancreatic cancer overall survival. It nearly doubled OS in the recent RASolute-302 trial.
And now that I’ve sort of gotten that out of the way for listeners, I’d love for you to maybe just kind of wax poetic, talk about what this drug means to the field, and why it’s so important and why it has taken the world by storm. And maybe later, maybe this is too big of a question all at once, but sort of the story behind the development of the drug as well.
Robert Mayer: Sure. Well, it’s a pleasure to be here. Pancreatic cancer has been viewed as an enormous scourge in the field of oncology. I particularly recall a reasonable number of physicians in whom the diagnosis was made and they themselves were reluctant to undergo any form of treatment, feeling that the disease represented a hopeless situation.
The presentation that we heard about an effective RAS inhibitor, we heard in ASCO several weeks ago, dispels that notion because it tells us that pancreatic cancer just as was once the case with melanoma was once the case with renal cell cancer may turn out to be treatable utilizing tools that we didn’t even know existed not so long ago.
Jacquelyn Cobb: Yes. Yes, absolutely. I mean, there’s sort of a different directions I can go, but since you mentioned that, I mean, would you talk a little bit more in depth about the specifics of what it looked like when you were treating GI cancers when you started and sort of what it looks like now? I mean, how do you reconcile these two different worlds? I mean, what were you treating GI cancers, pancreatic cancers with?
Robert Mayer: I think GI cancers fell under the domain of surgeons for many, many years. In contrast to the so-called liquid tumors, leukemia and hemopoietic malignancies, myeloma. A chance to cut became a chance to cure. Certainly that was the case in colon cancer. Certainly that was the hope in gastric cancer.
When I became interested in GI cancer, which was around 1975, it was a time that the National Cancer Institute supported a multidisciplinary, multi-modality group to explore various options in GI cancers, which included colorectal and gastric cancer, but also pancreatic cancer. That was known as the gastrointestinal tumor study group. It involved our group at Harvard, the group at Yale, the Mayo Clinic, Roswell Park, the University of Chicago, Georgetown, UCLA. Major institutions.
And candidly, we didn’t totally know what we were doing. There was early data at that time that suggested that prophylactic postoperative chemotherapy was effective in breast cancer.
There were no such data in colon cancer, which is the most common of the GI malignancies.
We had no tools, say like CT scans, to even identify or diagnose these tumors at an early time. Colonoscopy was a big deal. Making a diagnosis of a pancreatic cancer often was restricted to the presence of metastatic disease because there was no scan, no blood test that showed that there was something awry in the pancreas that was in the back of the abdomen and that didn’t change for quite some time. So the aura developed that this was something that just couldn’t deal with.
And we tried, we made the analogy to colon cancer. The disease was treated with 5-fluorouracil–based therapy, not all that effectively. There was an operation, the Whipple resection, which now technically is done on a regular basis. But 45-50 years ago, there were some institutions that felt that the operation caused more harm and benefit because of the side effects, because of the recurrence rate that seemed to be inevitable even when such an operation was carried out.
So, the notion was that if you took a hundred people with pancreatic cancer, maybe one out of 24 or 5% would still be with us at five years.
A bunch of things started to happen after that. First people became interested in learning why this was such a difficult disease to treat. For example, there was this desmoplastic scarring sheet almost protecting the tumor from any type of radiation or surgery. We still don’t have an answer for that, but that explains in some ways why radiation treatment was not as effective here as it was in colon cancer.
We learned that people who were soon to be found to have pancreatic cancer often developed diabetes, glucose intolerance, what we now call type two diabetes, probably because there was some irritation and inflammation in the pancreas, even though until the CT scans became readily accessible in the mid 1980s, we couldn’t really see that.
In the 1990s, we had a new drug. We had gemcitabine, Gemzola, which was shown to be better than 5-FU in a seminal study that was published in the Journal of Clinical Oncology and there was a great deal of hope that the use of gemcitabine would make a major difference.
As it turned out going to maybe 2010, 2011, the French investigators, maybe being more traditional in their thoughts, combined all the drugs that were then effective or used in colon cancer—like 5-fluorouracil, oxaliplatin, irinotecan, and leucovorin—into FOLFIRINOX. When they compared that to gemcitabine, there was a benefit both in metastatic disease survival and there was a benefit in giving it prophylactically as an adjuvant treatment.
Similarly, gemcitabine, along with nab-paclitaxel, turned out to be effective. So, there was attention that was being paid to this. There also was a great deal of interest in the patient community and formation of foundations. The Lustgarten Foundation, which supported the notion that young investigators should put their creative efforts into studying this disease.
Pancan, which provided patients a great deal of benefit and health, and through those efforts it became clear that 90% of pancreatic cancers harbored a mutation, a mutation in the KRAS gene. That was helpful in learning more about the biology of the disease. It was tantalizing to think that inhibiting that might do something beneficial for patients so affected, but a decade or more of attempts at developing inhibitors of the KRAS gene that would have any effect on pancreatic cancer turned out not to be fruitful and the RAS mutation of pancreatic cancer developed the reputation as being as being undruggable, but that doesn’t mean the work should stop and there have been more and more creative attempts at finding different ways of early detection, of being able to biopsy this disease at an earlier stage, of giving chemotherapy before operating—strategies that were not going to markedly improve survival outcomes, but certainly to push the gate a little bit further.
And it made pancreatic cancer perhaps along with glioblastoma with brain tumors, but two most difficult problems that we as medical oncologists and cancer doctors have to deal with making this recent observation so exciting. Now we have a tool. We have something much easier for patients in theory to utilize—no four-drug infusions, no neurotoxicity, taking a pill once a day. It’s a whole new game, the rules have changed and now with the data that’s beautifully presented by my colleague Dr. Wolpin at ASCO a few weeks ago, showing an unequivocal superiority for the RAS inhibitor versus alternative chemotherapy in second line treatment.
Now the issue of what happens if you give the RAS inhibitor before an operation, could you shrink the tumor, could you convert somebody who would otherwise be destined to recur or have an incomplete operation? Could you give the drug after the operation as well? What happens if you fail or the disease returns? Is this the only RAS inhibitor of its class?
We certainly learned in the world of lung cancer and in the world of chronic myelogenous leukemia that the first drug that seemed to work didn’t necessarily represent the best that would ever come. On the other hand, it opened the door to new things and those new things have been amazing to watch.
I’m giving a talk to a group of students who are entering Harvard Medical School this summer who are going to spend the month before they matriculate, before they enter the school, and spending time at Dana-Farber using oncology and care and science as a metaphor for what contemporary academic medicine can be and just thinking of how we have proceeded, progressed from sort of blindly utilizing non-specific compounds, which can be highly toxic, putting the correct key into the correct lock and opening the door is something… to really relish.
Jacquelyn Cobb: That’s wonderful. Thank you. And I think that you touched on it so well, this idea that there were some drugs, gemcitabine, the FOLFIRINOX regimen, that what you said, they did demonstrate some superiority, like you said, but this daraxonrasib is the first time we’ve seen like a sort of a… How would you describe that? It’s the first time we’ve seen like a real … It doubled OS.
Robert Mayer: Well, you look at curves. I used to be on an editorial board where the editor-in-chief said, “If you’re comparing two survival curves and you can’t put two fingers between them, statistics don’t matter. It had no clinical real bearing.” It was the two finger rule.
This is a whole fist, your whole hand between the two curves. This is not something that you have to have a masters or doctorate degree in statistics to understand. This is something that people, the community, the society should appreciate comes from years and years of swings and misses, foul balls, and finally a direct hit that really will, I very much believe, change the outcome for patients in the future with this disease.
Jacquelyn Cobb: Yeah, absolutely. And I’m already seeing combinations I feel like are a huge sort of future direction that people are talking about. Because that is the concern with RAS, resistance develops; right? Is that sort of the challenge with RAS? Am I misremembering that?
Robert Mayer: Well, I don’t think we really know that.
Jacquelyn Cobb: I guess that’s true.
Robert Mayer: Well, what we know is that people with pancreatic cancer who have previously been treated benefit from this therapy. Would adding a RAS inhibitor to FOLFIRINOX make FOLFIRINOX more potent? I don’t know. We’ll learn.
As I was saying before, with such a high response rate in a disease, in a condition, where even benefits were in the notion of extending median survival a month or two, but not really necessarily taking away symptoms and making a big lump shrink to something much smaller, potentially resectable, potentially curable, that may not be the case anymore and we need to move on that. So I think the hors d’oeuvre table has a lot of options here and I’m hoping that a lot of young, bright people who are entering this field will see this as a wonderful opportunity for us to move forward.
Jacquelyn Cobb: Yeah, absolutely. And I mean, you’ve touched on this and you’ve said it sort of in several different ways. I just want to give you a proper platform to really just kind of talk about it personally. What is it like as an individual to have entered the field when CTs weren’t even regularly used, you didn’t even know like what you just described and now we have this. What is that whiplash like?
Robert Mayer: It is to me blowing away the fog. To meet as I do regularly patients who have been sent because there’s a lump in their pancreas or they’re known to have pancreatic cancer or they have metastatic disease that has not benefited from treatment and try to inject positive hope and goals using all the tools that our palliative care colleagues have so wonderfully defined is frustrating.
I come from a generation where leukemia was untreatable and bone marrow transplantation was some sort of a mystical process and now we have CAR T-cells, we have so many ways of marshaling tools to reduce the cancer burden. To have that happen with pancreatic cancer is just hard to put into words. Now, as with other conditions that we treat when patients come, we’ll be able to give them options, plans, steps. It may not necessarily be that we can cure, but we can prolong survival, enhance quality of life, reduce time that they have to come to receive toxic systemic parenteral intravenous therapy. All things that really matter, so that they can go and be at high school, college graduations, and family celebrations, and function and do all the things that they otherwise would like to do. That has never been something that happened with pancreas cancer.
Most people who—at least I’ve treated over the years—been cured of pancreatic cancer have been found to have it by accident. For some reason they had a CT scan, they were in an auto accident, they had a broken rib—whatever it might be—something was found and something could be done at a time when the disease really hadn’t really gotten a hold of the patient. But there was no screening test up to now, and even this sort of treatment, which is such an exciting event, is maybe hopefully going to induce even more effort to try to learn how to find the disease at an earlier time, which I know people are working very hard on, but is easier to say than to do.
Jacquelyn Cobb: Absolutely. Well, let me just take a look at my questions. I mean, if you’re up for it and we have a little bit of time, I would love to sort of shift and talk just about your personal history and sort of how you got into cancer research at Dana-Farber. I mean, I’m sure that you have sort of a… It doesn’t have to be focused on RAS necessarily is what I’m trying to say
Robert Mayer: Well, I was lucky enough to come out of my medical residency and spend three years, three very formative years, at the National Cancer Institute. It was a time in the early 1970s when treating cancer was thought to be sort of a feudal effort, maybe using hormone therapy for breast cancer, and even increasingly then for prostate cancer, but for many of the diseases that we treat, if you could not resect it, you couldn’t deal with it. I remember at that time there was a great deal of excitement about finding high dose methotrexate as a treatment, as a therapy for teenagers who had bone cancer, osteosarcoma, but they nearly always ended up having an amputation and now these patients are able to have pre-surgical treatment of the operations are much less radical and life changed.
But the notion came, from my generation at the NCI, that you could do something about cancer if you could understand it better. Maybe people were studying how the kidney functioned or the lung transferred oxygen, and maybe they were a little ahead of the game, but that didn’t mean that people who were interested in why normal breast ducts become malignant and what to do about it shouldn’t devote their career to it. And while I was at the National Cancer Institute, the early studies, very courageous studies, of avoiding disfiguring mastectomies, removing the lumps, using other tools, radiation, chemotherapy, hormone therapy, was able to extend life and cure many, many people.
I had been at the NCI for two, two and a half years when I had a call from a former professor of mine, a hematologist at Harvard who said, a man by the name of Emil Frei, was going to move from MD Anderson to Boston to become the director of what would become the Dana-Farber Cancer Institute, cancer center at Harvard. Most academic medical centers did not have a cancer center in those days and then I ought to think about moving back to Boston, where I had been at medical school, and getting in on the ground floor. And that’s exactly what happened.
I came here with a few other people from the National Cancer Institute and we began one of the first medical oncology fellowship programs. We reached out to all the surrounding hospitals and began clinical studies and the science and the tools developed at the same point and sort of being in the right place at the right time. And GI cancer, that GI tumor study group, indeed turned out to be a major step for me personally because I learned so much. Being injected as a youngster, if you will, with senior people in the field. Giants. Charles Moertel from the Mayo Clinic. Groups from Roswell. It was a wonderful learning opportunity for me.
As the years passed, just more barriers fell and they have fallen even more and this experience with pancreatic cancer probably is as exciting as anyone could imagine. I’m impatient to see what the next three, four, five years have.
Jacquelyn Cobb: Yeah, absolutely, absolutely. Well, thank you so much. This has been incredible. Is there anything… I feel like there must be more that I didn’t ask the right question. I want to hear more about sort of what it was like and stuff like that, but obviously I don’t want to take up too much of your time. So is there anything that we missed that you feel is really necessary to this conversation?
Robert Mayer: Well, you tell me what you’re interested in and I’ll fill it in.
Jacquelyn Cobb: Well, I think my only lingering question is sort of the NCI RAS initiative and how that played into the development of RAS because of daraxonrasib and what you said about how it was undruggable. That’s sort of what I was taught in school was that RAS is undruggable, KRAS is undruggable, it’s a golf ball, you can’t do it. And then I do know, of course, it was at UCSD that they discovered that it technically was druggable, but I guess what I’m not sure about is the link between Revolution Medicines, daraxonrasib—I haven’t gotten it down—and the broader push to try to target KRAS in pancreatic cancer.
Robert Mayer: I think it’s important for us all to appreciate that the observation about the efficacy of this new RAS inhibitor didn’t occur by accident. It occurred in large part because of federal funding over many years, primarily from the National Cancer Institute. It emerged from partnerships between federal agencies, academic centers, and biotechnology institutions, and laboratories. Those sort of partnerships need to continue.
I think that we as a community are obligated to acknowledge that there’s nothing mystical about how science is conducted. It’s a long slog of wonderfully committed, amazingly talented people who collaborate. I know that many of the efforts that they undertake are not going to be successful. But see as the goal, improving the health of the people we serve, now more than ever, the recognition of the support of fundamental basic research as the starting point for what will prove to be hopefully a major change in the outcome for patients with a dreaded disease. It has to continue and we as a society need to embrace that.
Jacquelyn Cobb: And I guess my last question that I was thinking of, and I don’t know if you’ll be able to answer it, but obviously I was kind of clued into sort of the RAS, the undrugability, stuff like that. Just because that’s what I had learned in school. Looking out at the field now, is there any other sort of almost answered question or something analogous to a RAS breakthrough that might be on the horizon that we should be paying attention to?
Robert Mayer: I think that the notion of harnessing the immune system to reduce tumor burden has been shown in patients with lymphoma, and myeloma, and some forms of leukemia to be extremely powerful.
On the other hand, what would be even more powerful from a population based vantage point is a means of applying those same principles to more common solid tumors such as the non-small cell lung cancer that occurs in non-smokers that still is appearing very frequently, such as some forms of gastric and gastroesophageal cancers that overexpress amplification of HER2 and may possibly be able to be harnessed in that same way.
I think that we need to think out of the box both in terms of funding and in terms of priorities to explore these novel and exciting therapeutic avenues and just remind ourselves that this wouldn’t have happened in pancreas cancer if people had given up.
I think another area where some early and preliminary data are intriguing is in the treatment of glioblastoma and we need to gather more information about that dreaded disease as well.
I think it’s sobering that many of the young faculty who are so appropriately engrossed in the genomic and molecular, and now AI studies, that are so prevalent have perhaps lost or never had the chance to appreciate the courage of some of the early pioneers in oncology. I think at my institution, Tom Frei [Emil “Tom” Frei III] came from MD Anderson, and before that, the National Cancer Institute. And what he really brought was optimism. He brought a sense of, “We can do this. It may take time, but we can do it and we’re going for cure.”
And then there were people like Bernie Fisher. Bernie Fisher was the founder of the National Surgical Adjuvant Breast and Bowel Project based at the University of Pittsburgh. As a surgeon, he had performed laboratory studies that indicated that big disfiguring operations in animal models for breast cancer didn’t achieve a better outcome because survival was defined by spread or lack of spread of tumor cells to distance sites and he was able, with enormous commitment, to perform one randomized trial after the other—later with Norm Wallmark as well and their colleagues—which greatly enhanced the quality of life and the fear that many women with a lump in their breast had and probably got many of them to go see a physician at a time that their disease was potentially curable than it might have been if they had been afraid and ignored it. All because Fisher’s work showed that this was something that wouldn’t create just such a big anatomic gap in their physiognomy.
So I think we really need to recall these people who are such giants in the field. They stimulated me. I hope they will continue to be remembered for the giant they are.
Jacquelyn Cobb: Yes, absolutely. And we’ll do our part with that. Maybe all med students need, or all oncology med students need a history of oncology class. Because I think you’re right, it’s really incredible to see the progress over the last, what is it now? 60 years? 70 years? Since the National Cancer Act.
Robert Mayer: ASCO started in 1964. I joined in 1975. I’m a 50 year person and it becomes part of who you are and it has been, for a career, it’s been a very great thrill to watch your trainees assume major leadership roles. It makes somebody with gray hair or no hair very proud and I feel very strongly about that.
The present director of the NCI is my second trainee who has been in that role. It’s something special. The president of Dana Farber now was a trainee. He’s marvelous. Just spectacularly capable and multi-talented person.
And I also am so impressed how the best and the brightest these days are moving into or have moved into the study and treatment of cancer because that’s where the action is. That’s where the cardiologists are learning from genomic studies that are being done for cancer and the naysayers in the past from traditional academic medicine who thought that poisoning people with cancer with chemotherapy wouldn’t go anywhere. Probably they were right in the shorter term, but when you didn’t draw attention to the possibilities and options and move ahead, you wouldn’t have learned anything. And so this has all been a tremendously rewarding experience and to see this progress in pancreatic cancer is something really special.
The Cancer History Project is an initiative of the Cancer Letter, the leading source for information on the issues that shape oncology since 1973. Learn more and explore our archives at cancerhistoryproject.com.